Gross failure in basic care by midwives led to death of Ida Lock, coroner rules
Ida Lock suffered a serious brain injury due to a lack of oxygen around the time of her delivery at Royal Lancaster Infirmary in 2019.

A gross failure by midwives to provide basic medical care led to the death of a baby girl, a coroner has concluded.
Ida Lock suffered a serious brain injury due to a lack of oxygen around the time of her delivery at Royal Lancaster Infirmary.
She was transferred to intensive care at Royal Preston Hospital’s neonatal unit where she died a week later on November 16 2019.
In April 2020, a report from the independent Healthcare Safety Investigation Branch (HSIB) identified numerous failings in the care of Ida which contributed to her death, the hearing at County Hall, Preston, had previously heard.

Midwives had failed to identify an abnormally slow foetal heart rate after Ida’s mother, Sarah Robinson, attended in early labour and then following birth there was ineffective resuscitation, the HSIB concluded.
But an earlier internal “root cause analysis” from the hospital in January 2020 found no issues and praised the “great cohesion and communication” shown by staff in the delivery suite.
Ida’s parents, Ms Robinson and Ryan Lock, from Morecambe, complained to University Hospitals of Morecambe Bay NHS Foundation Trust (UHMBT), which runs the hospital when they saw the two reports that they compared to “night and day”.
Delivering a narrative conclusion on Friday, HM Senior Coroner for Lancashire, Dr James Adeley, said: “Ida was a normal child whose death was caused by a lack of oxygen during her delivery that occurred due to the gross failure of the three midwives attending her to provide basic medical care to deliver Ida urgently when it was apparent she was in distress”.
He added her death was contributed to by the lead midwife’s “wholly incompetent” failure to provide basic neonatal resuscitation for Ida during the first three-and-half minutes of her life, which further contributed to the infant’s brain damage.
Dr Adeley identified eight missed opportunities by midwives to alter Ida’s clinical course.
UHMBT was the subject of a damning report in 2015 that found a “lethal mix” of problems at another of its maternity units at Furness General Hospital that led to the unnecessary deaths of 11 babies and one mother between 2004 and 2013.
The Morecambe Bay investigation, chaired by Dr Bill Kirkup, uncovered a series of failures “at every level” from the unit to those responsible for regulating and monitoring the trust.
Dr Adeley said: “Clinical governance is a framework through which NHS organisations and their staff are accountable for continuously improving the quality and safety of patient care.
“Clinical governance is also intended to ensure that healthcare professionals adhere to the highest standards of care and that the appropriate systems and processes are in place to monitor clinical practice.
“Ida’s death and subsequent investigation is a damning indictment of an ineffective, dysfunctional and callous system that has failed this family at every opportunity presented to it.”
The coroner said he would be filing a prevention of future deaths report with the health trust which will be copied to, among others, Health Secretary Wes Streeting and the chief coroner.
He said: “In this case I consider the clinical governance arrangements at the trust together with the culture, require that I take action to reduce the risk of deaths to mothers and children created by those circumstances.
“However, it is apparent from the evidence of Dr Kirkup (at the inquest) and the increasing number of inquiries into significant shortcomings in maternity units, that this is a national issue and consequently I will also be filing a prevention of future deaths report with the Secretary of State for Health and the chief coroner.”
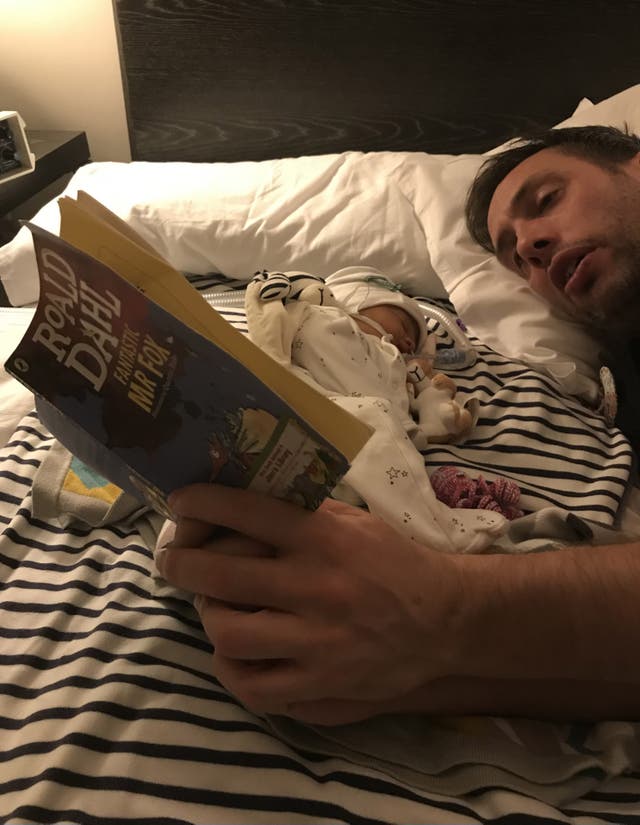
Following the inquest Mr Lock, speaking alongside Ms Robinson, said: “Words truly cannot express how heartbreaking it was to lose Ida and there is not a single moment that passes when we do not think of her and what she may have become.
“Today the coroner found neglect had led to the death of our beautiful baby girl. The coroner found there had been a litany of serious, preventable failures in medical care that Ida received.
“In June 2020 we spent hours and days preparing a letter (to the health trust) listing our questions and concerns. We were casting around in the dark, trying to understand what happened.
“We have still not received any response to that letter.
“We still don’t know why the trust were not open, why they were not candid, why they didn’t tell us what had happened.
“Hopefully, Ida is no longer a hospital number and her name will be used to implement change and at the very least influence parents to question, to push and to understand what has happened.
“The answers today will not bring our daughter back but it will hopefully stop any other family having to go through what our family have.
“It should not be a test of endurance for bereaved and bewildered parents to work out what happened to their child. Hopefully, today is the start of healing and we can grieve differently for Ida.”
In his summing up, Dr Adeley noted that a senior midwife completed an incident report – the first step in the clinical governance process – that was “at best misleading and at worst a significant misrepresentation of the facts relating to the treatment provided to Ms Robinson and Ida and their clinical conditions”.
He said the report was “disingenuous” in that it portrayed Ida’s delivery in a manner that obscured the actual clinical picture of Ida’s delivery, misrepresented the resuscitation to such an extent that it was not an issue and gave the wrong impression to those undertaking a “rapid review” of the case and the root cause analysis (RCA) that followed.
The coroner said: “In respect of the trust’s clinical governance investigations of the rapid review and RCA, these clearly demonstrate the failures identified by the Kirkup Report and were investigated by either untrained or poorly trained staff and characterised by superficiality, brevity and protectiveness to midwives with grossly deficient inputs from clinicians.”
Giving evidence at the inquest Dr Kirkup said the RCA report was “wholly inadequate, fragmented, incomplete and defensive, which was an attitude that got in the way of learning lessons from adverse events”.
He said it showed “nearly all the same features identified” in his 2015 inquiry.
Dr Adeley said UHMBT maintains it was Royal Preston Hospital’s responsibility to identify the coroner of Ida’s death – despite nothing unnatural occurring during her treatment there.
Mr Lock and Ms Robinson wrote to UHMBT in October 2020 to ask them to refer the death to the coroner, in light of the HSIB’s findings, but received no response and instead weeks later reported the death themselves to Dr Adeley’s office.
The coroner said: “Consequently, the trust avoided notifying any external agency with any meaningful information that would have resulted in external scrutiny of trust processes and the care provided for almost a year after Ida’s death.
“Ms Robinson and Mr Lock have received an explanation as to what happened to Ida at an inquest, although the route they have had to travel must have extracted an appalling cost on their family.”
In a statement, Tabetha Darmon, chief nursing officer of UHMBT, said: “Losing a child is tragic and our heartfelt condolences go out to Ida’s parents, family and loved ones. We are truly sorry for the distress we have caused.
“We accept that we failed Ida and her family and if we had done some things differently and sooner, Ida would still be here today.
“We also acknowledge the additional upset caused to Ida’s parents and family as a result of the way investigations into Ida’s death have been conducted since 2019.
“For that, we are truly sorry.
“We take the conclusions from the coroner very seriously and have made a number of the improvements identified during the inquest.
“We are carefully reviewing the learning identified to ensure that we do everything we can to prevent this from happening to another family.”




